Rib issues—often overlooked!
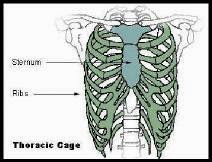
The human rib cage, also known as the thoracic cage, is a bony and cartilaginous structure which surrounds the thoracic chest and supports the pectoral (shoulder) girdle, forming a core portion of the human skeleton. A typical human rib cage consists of 24 ribs, the sternum, costal cartilages, and the 12 thoracic vertebrae. It, along with the skin and associated fascia and muscles, makes up the thoracic wall, and provides attachments for the muscles of the neck, thorax (mid back), upper abdomen, and back.
The human rib cage is a component of the human respiratory system. It encloses the thoracic cavity, which contains the lungs. An inhalation is accomplished when the muscular diaphragm, at the floor of the thoracic cavity, contracts and flattens, while contraction of inter-costal muscles lift the rib cage up and out. The ribs must move outwards and upwards with the inhalation. With the exhalation the rib move in the opposite direction.
Many people have rib misalignments and they occur as a result of coughing, sneezing, faulty postural mechanics, abnormal spinal curves, asthma, allergies and childhood diseases such as: Scheuermann’s disease, pneumonia, bronchitis, scoliosis.
You will often feel pressure on the chest, in the middle back, lower neck. Sometimes you can experience a sharp pain when breathing in or out.
This can be treated with a combination of: chiropractic adjustments, Active Release, working on the postural faults, and stretching.
Adhesions—what are they?
An adhesion is a band of scar tissue that binds 2 parts of your muscle, tendon, ligament or nerve together. Theses 2 parts should remain separate. Adhesion may appear as thin sheets of tissue similar to plastic wrap or as thick fibrous bands. Adhesions develop as the bodies attempt to try to repair itself. This normal response can occur after surgery, falls, repetitive strain on a body part, faulty body mechanics, incorrect posture while sitting, other traumas, and radiation. Repair cells in the body cannot tell the difference between normal tissue and themselves. They then connect the 2 surfaces. Visualize a spider web and the adhesions look somewhat like this. The normal tissue is supposed to appear linear in nature.
Are you not flexible?
Here’s the clincher: Reduction of supraspinatus function results in compensation from the remaining muscles of the rotator cuff. The subscapularis muscle works hard to prevent the humerus from riding upward towards the acromial roof, while the remaining rotator cuff muscles expend greater energy to stabilize the joint. Overuse of the muscles lead to an excess build-up of metabolites, which the circulatory system cannot transport effectively. The accumulated metabolic waste products soon gel together forming adhesions, the scar tissue that entraps the muscles, ligaments and nerves between fibres. The cascade doesn’t stop here. In fact, with repeated exposure to micro-trauma, the network of soft tissues of the shoulder complex and spine become affected. Joint capsule inflammation, nerve, vascular and lymphatic supply, are swiftly altered to accommodate for the changes. Ultimately, something has to give pain and dysfunction prevent the athlete from performing with maximum efficiency.
Supraspinatus tendonitis is only one example of this mechanical imbalance. In fact, dysfunction of any muscle or complex attaching to the shoulder joint may stimulate a similar cascade of events.
One of the most effective forms of treatment for repetitive strain injuries is a soft tissue therapy called the Active Release Technique (ART). ART in conjunction with neuromuscular re-education is one of the most effective combinations of treatment available. Chiropractic and massage are beneficial to ensure the functional integrity of the surrounding elements work properly as well!
What’s up with my shoulder?
Why shoulder injuries are so common among triathletes.

Shoulder injuries are common with triathletes, either as a result of direct contact from a collision or fall, or from repetitive overhead motion. By far, the majority of cases stem from repeated stresses that, due to the accumulative effects, lead to mechanical impingement and micro-trauma.
Improper stroke technique is the culprit for most overuse injuries of the shoulder joint in freestyle swimming.
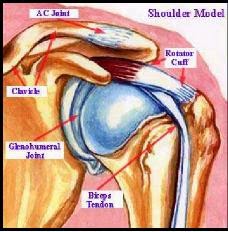
Supraspinatus tendonitis, with or without subacromial bursitis, is renowned in swimmers, hence the name swimmer’s shoulder. The reason why? It’s as simple as looking at the anatomy of the shoulder joint. As a group, four muscles attach to the scapula and stabilize the shoulder by compressing the humerus into the glenoid fossa. All four muscles join the scapula to the head of the humerus, with each muscle running a slightly different course to get there.
Supraspinatus makes up one of the four rotator cuff muscles. The supraspinatus muscle is unique in that its tendon must pass under the roof of the acromium, sandwiched between the subacromial bursa and the tendon of the long head of biceps brachii to attach to the humerus.
Repeated overhead motions render the supraspinatus tendon susceptible to impingement between neighboring structures. Before you know it, the supraspinatus tendon is irritated and inflamed becoming a nagging source of pain and discomfort.
FEATURE STRETCH: Low Back Twist

Lie on your back with your arms out from your sides and bend one knee. Move your bent knee across your body to the opposite side, trying to touch the floor on that side while keeping your shoulders flat on the floor. Look to the opposite side, away from your bent knee. Hold the stretch for 30 seconds and repeat 3 times. Repeat on the other side.